Table of Contents
TLDR: Healthcare organizations investing in remote patient monitoring are building infrastructure that supports CMS reimbursement, reduced readmissions, and better chronic care outcomes. As connected care continues to expand, RPM software is becoming a strategic investment for modern healthcare delivery. This guide covers what to build, how to build it, and the decisions that matter most.
Hospitals that implemented remote patient monitoring programs during COVID never went back, and the numbers explain why. Digital health tools have become a routine part of modern healthcare workflows, extending care beyond traditional clinical settings. That shift is about clinical outcomes, CMS billing viability, and the economic pressure of value-based care. Remote patient monitoring is now a core infrastructure decision for health systems and health-tech teams alike. This guide explains architecture, features, compliance requirements, and what to build first.
Remote patient monitoring collects physiological data from patients outside clinical settings using connected devices and transmits that data to care teams for clinical review and action.
It differs from telehealth in one important way: RPM is passive and continuous. Telehealth is an appointment. Remote patient monitoring is always-on infrastructure.
RPM software manages device connectivity, data ingestion, alert generation, and EHR documentation. Telehealth RPM integration combines patient data tracking with virtual consultations. The difference matters for billing.
CMS RPM billing codes (CPT 99453, 99454, 99457, 99458) require documented device readings and clinical time, which a remote health monitoring system tracks automatically. Telehealth platforms do not.
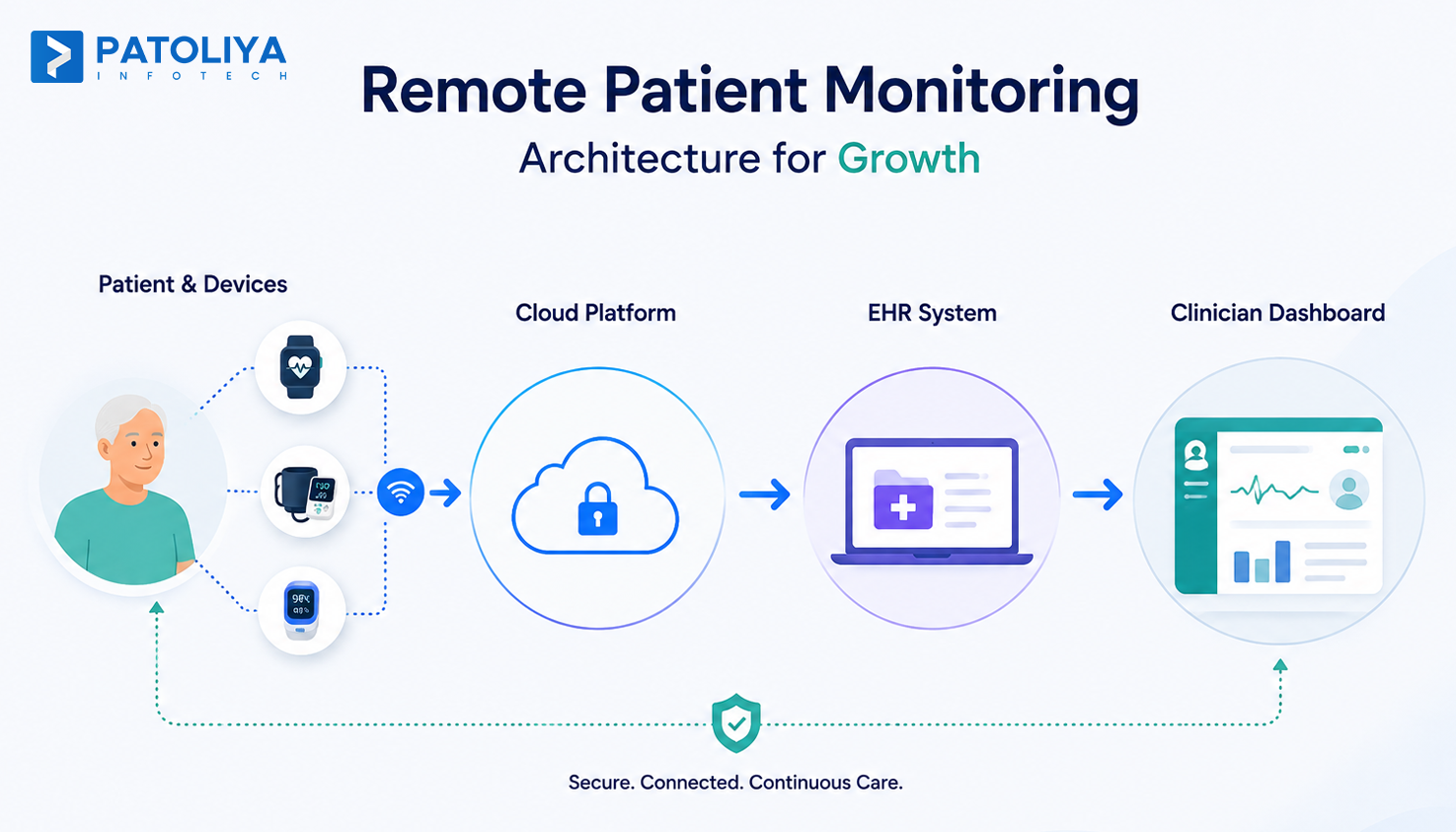
| Step | What Happens |
| 1. Collection | Wearable IoMT sensors and connected devices capture biometric readings |
| 2. Transmission | Data moves via Bluetooth or cellular to a cloud gateway |
| 3. Processing | Rules engines or ML models flag abnormal readings |
| 4. Review | Clinicians see alerts in dashboards; data syncs to EHR |
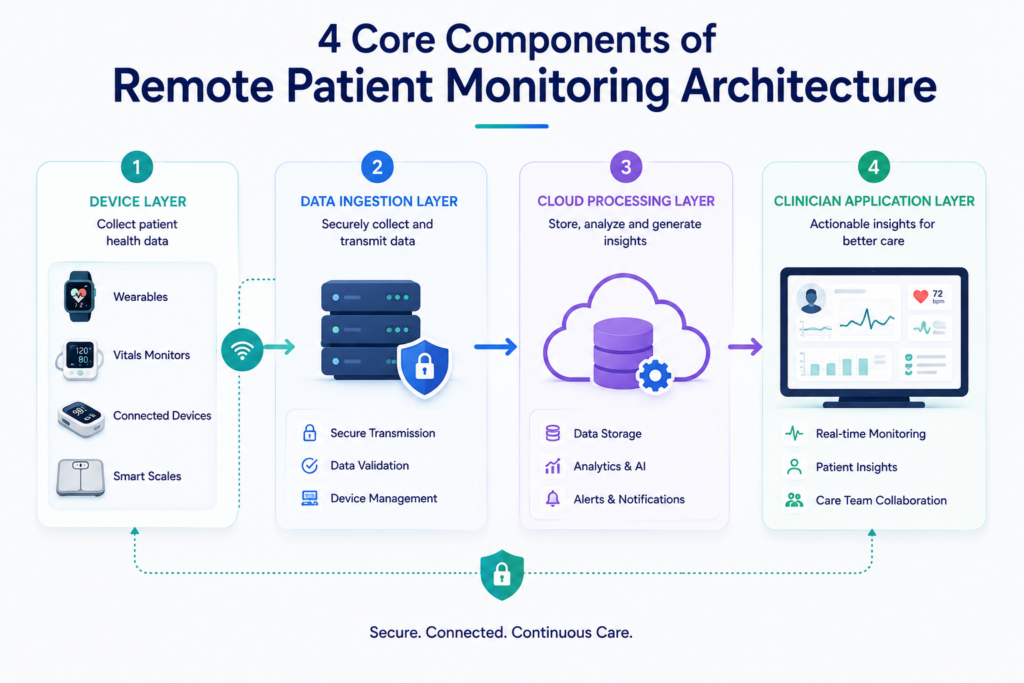
A production-grade remote health monitoring system is not a single application. It is four distinct technical layers working together. Each layer for Remote patient monitoring has its own scalability and compliance requirements. Teams that treat this as one monolith spend months untangling it later.
Remote patient monitoring programs fail at scale when feature decisions are made without clinical workflow input. The following features are required for a functioning RPM software product. Optional features are covered in the MVP section below.
The patient app needs device pairing, health data visualization, medication reminders, and secure messaging. Onboarding friction is the biggest driver of early dropout. A patient adherence app must reduce cognitive load, not add it.
Clinicians need monitoring views sorted by risk, alert management, and integrated clinical notes. In Remote patient monitoring, Dashboards that surface 200 patients without prioritization create alert fatigue. Risk scoring should surface the top 10 to 20 patients who need action today.
Threshold-based alerts cover basic cases. A well-designed escalation engine routes alerts based on severity, time of day, and role. Alert fatigue is the silent killer of remote patient monitoring programs. Most programs that fail cite alert volume, not device issues.
CMS RPM billing 2026 codes require documented device readings for at least 16 days per month and tracked clinical time. Built-in time logging and audit trails are not optional. They are the financial foundation of the program.
Clinical outcomes reporting and program performance dashboards help organizations justify expansion. Remote patient monitoring programs need data to prove ROI to hospital leadership and payers.
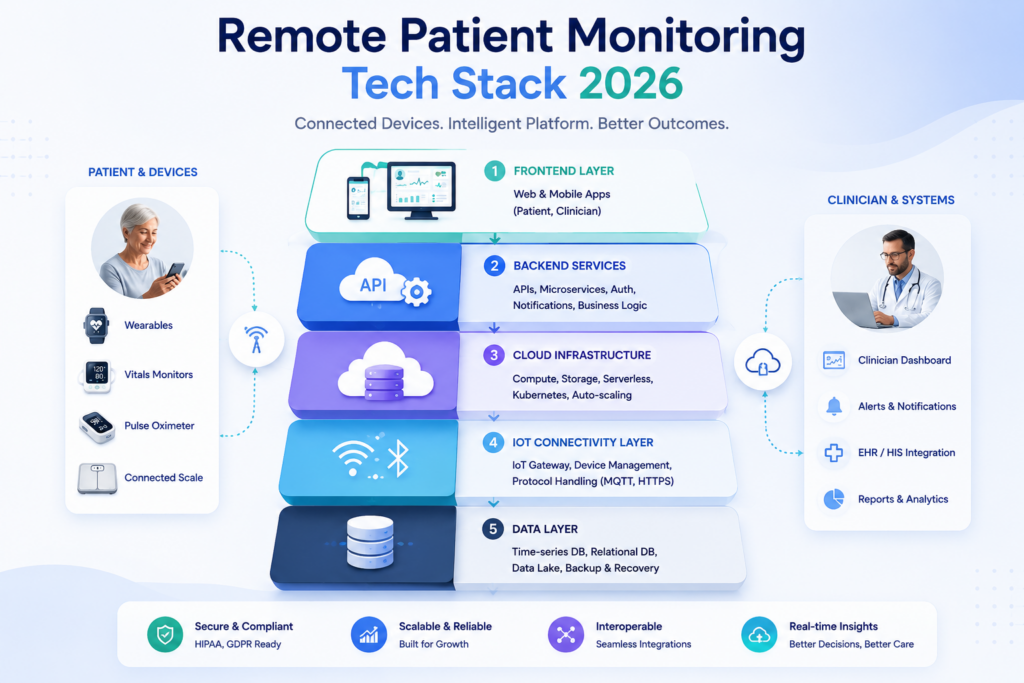
Technology choices in remote patient monitoring software development compound quickly. A stack that handles 500 patients struggles at 50,000 without architectural rework. Choose for the scale you intend to reach, not the scale you are at today.
React and Next.js handle clinician dashboards well. Flutter or React Native serve cross-platform patient apps efficiently.
For backend, Node.js and Python work for most teams. Java Spring Boot suits organizations with existing enterprise Java infrastructure. Choose what your team knows and can maintain in Remote patient monitoring.
PostgreSQL handles relational data. InfluxDB or TimescaleDB handle time-series device readings more efficiently. AWS and Azure both provide HIPAA-eligible infrastructure.
For Remote patient monitoring, the key decision is not which cloud; it is whether your team has built healthcare-compliant cloud environments before.
Bluetooth Low Energy is the standard for consumer health devices. MQTT handles high-frequency device messaging efficiently.
WebSockets maintain persistent connections for real-time dashboard updates in Remote patient monitoring. A device-agnostic integration layer avoids vendor lock-in and future-proofs your remote health monitoring system as new devices enter the market.
Apache Kafka handles event streaming at volume. Real-time analytics platforms like Grafana surface operational metrics.
Observability tools catch latency issues before they affect clinical workflows in a remote patient monitoring environment.
HIPAA compliance in RPM software is an architectural commitment. Teams that bolt security on after building functionality spend three to six months reworking core systems. Build compliance into data models, API design, and access control from day one.
AES-256 encryption at rest and TLS 1.2 or higher in transit are the baseline. Key management requires a dedicated KMS.
Any remote health monitoring system that stores PHI without proper key rotation is a HIPAA violation waiting to happen.
RBAC must map to actual clinical roles: patient, care coordinator, nurse, physician, and administrator.
Each role has different data access and action permissions. A care coordinator should not have the same access as an attending physician in your remote patient monitoring software.
Every PHI access, modification, and export must be logged with a timestamp, user ID, and action type.
HIPAA requires audit log retention for a minimum of six years. Log your remote patient monitoring system's access patterns and monitor for anomalies. Logging without monitoring is not compliance.
Multi-factor authentication is required for all clinical users. SSO integration with hospital identity providers reduces friction and improves security posture. Session timeouts must be enforced across all RPM software interfaces.
The three most common mistakes in Remote patient monitoring are: no audit logs on read operations, missing Business Associate Agreements with cloud vendors, and unencrypted device data in transit before it reaches the cloud gateway.
Remote patient monitoring data has limited clinical value if it lives outside the EHR integration. Clinicians document in Epic or Cerner. If RPM readings do not appear there automatically, they get ignored. Integration is a foundational requirement. It is how RPM software becomes part of clinical workflow.
Why EHR Integration Is Critical
Without EHR integration, clinicians maintain two systems. That doubles documentation time. Remote patient monitoring data that does not flow into the patient record does not affect clinical decisions consistently.
FHIR R4 is the current standard for EHR-connected RPM data exchange. The key resources in Remote patient monitoring are:
| FHIR Resource | RPM Use Case |
| Patient | Enrollment and demographics |
| Observation | Device readings (vitals, glucose) |
| Device | Registered monitoring equipment |
| CarePlan | Monitoring protocols and goals |
FHIR R4 APIs are now required for certified EHRs under the 21st Century Cures Act, which significantly reduces integration friction for remote health monitoring system builders.
Most community hospitals still run HL7 v2. ADT messages handle patient admissions and discharges. ORM messages handle orders. Your remote patient monitoring software needs to speak both HL7 v2 and FHIR R4. Organizations that skip legacy support lose access to 40% of their potential market.
Mirth Connect is the most widely deployed open-source integration engine in healthcare. It handles message transformation between HL7 v2 and FHIR formats, routes messages to the right EHR endpoints, and provides audit logging. Most remote patient monitoring integration teams use it or a commercial equivalent.
Epic and Cerner each have proprietary APIs alongside FHIR R4. Budget four to eight weeks per EHR integration for a production-ready remote health monitoring system.
A technically sound remote patient monitoring platform fails if patients stop using it. Long-term RPM success depends on patient engagement, intuitive user experiences, and effective communication workflows. Engagement is an architecture problem, not just a UX problem.
The features in Remote patient monitoring with the highest adherence impact are:
Rules engines fire alerts when readings cross fixed thresholds. They are fast to implement and clinically transparent. Predictive models identify deterioration before thresholds are crossed. Both have a place in production RPM software.
Chronic disease monitoring programs benefit most from AI in these areas:
| Use Case | Clinical Value |
| Early deterioration detection | Intervene before hospitalization |
| Readmission prediction | Target post-discharge outreach |
| Chronic disease risk scoring | Stratify population monitoring |
Architecture for AI-powered remote patient monitoring requires a feature store, model serving infrastructure, and a feedback loop for model retraining. Regulatory considerations under FDA SaMD guidance apply to any AI that influences clinical decisions.
The most expensive mistake in remote patient monitoring product development is building too much before validating clinical workflows. An overbuilt MVP delays CMS billing eligibility and slows clinical feedback. Build the smallest set of features that qualifies for reimbursement and generates real patient data.
A market-ready RPM software MVP needs:
This set supports CMS billing from day one and validates the clinical workflow before further investment in Remote patient monitoring.
AI modules, advanced analytics, multi-device ecosystems, and complex care management workflows all belong in phase two for Remote patient monitoring. Building them first delays launch without adding reimbursable value to your remote health monitoring system.
A production-ready remote patient monitoring MVP with HIPAA compliance, EHR integration, and CMS billing support typically costs between $300,000 and $700,000 depending on team composition and device scope.
As remote patient monitoring programs grow, synchronous architectures break under device data volume. Event-driven architecture using Kafka or AWS EventBridge decouples ingestion from processing. Multi-tenant design isolates data by health system. A well-designed remote health monitoring system handles millions of daily events without reengineering the core. Build for this from the start.

Remote patient monitoring delivers measurable returns across three dimensions. Build your business case around all three.
Clinical Benefits: Reduced hospital readmissions and earlier intervention in chronic disease monitoring programs directly improve patient outcomes and quality scores.
Operational Benefits: Care coordinators manage larger patient panels with less manual outreach. Remote patient monitoring software automates what previously required phone calls.
Revenue and Reimbursement Opportunities: CMS reimbursement through CPT 99453 to 99458 creates a direct revenue line. A remote health monitoring system that tracks time and readings automatically captures every billable dollar.
| Metric | What It Measures |
| 30-day readmission rate | Clinical impact |
| Device adherence rate | Patient engagement |
| Monthly CPT billing volume | Revenue performance |
| Alert response time | Operational efficiency |
Patoliya Infotech builds remote patient monitoring platforms that are CMS-billable from day one, HIPAA-compliant by architecture, and integrated with Epic, Cerner, and legacy HL7 systems.
If you are scoping a remote health monitoring system and want a technical team that has done this before, let's explore what your program needs.
Remote patient monitoring is infrastructure. The organizations winning in connected care are not the ones with the best device hardware. They are the ones with the cleanest data pipelines, tightest EHR integration, and highest patient adherence. The technical decisions made today, around architecture, compliance, and clinical workflow, determine whether your RPM software scales or stalls. If you are ready to scope your build, let's talk.